
- Many orthodontic problems can be treated as easily in adults than in younger patients.
- Some additional risks may sometimes be associated with adult treatment but, in most cases, excellent results can still be obtained.
- Adults have no more growth so, if an imbalance exists between the size of the jaws, surgery of either jaw (or both) may be indicated to obtain a good relationship between the upper and lower dentition.
- In certain cases, a “compromise” or limited treatment designed simply to correct some aspects of a malocclusion may be considered while allowing a significant improvement in function and esthetics.
- “At my age, is it worth it?” Today, adults can expect to keep their teeth for a lifetime. The time when people expected to “lose their teeth when they were old” is over. Advances in modern dentistry and access to quality dental care now allow virtually all those who wish to have a functional and esthetic dentition throughout their lives to obtain it. Orthodontics is often one way to reach these goals.
- The possibility for an adult to undergo an orthodontic treatment depends more on his/her dental and general health than his/her chronological “age” per se.
The difference: adults vs teenagers
 If the health of your teeth, gums and bone that support your teeth is good, the orthodontic movement of teeth is virtually identical in adults than in younger patients. Certain differences in some adults may exist:
If the health of your teeth, gums and bone that support your teeth is good, the orthodontic movement of teeth is virtually identical in adults than in younger patients. Certain differences in some adults may exist:
- A fundamental difference between adults and children or teenagers is the absence of growth. When a significant skeletal imbalance between the jaws is present, it may be necessary to undergo a surgery to one or both jaws to obtain an adequate balance between the jaws.
- In younger patients, growth potential may be used to correct a skeletal imbalance, just like when one jaw is too advanced or too far back compared to the other one, for instance. (See the section on malocclusions for examples.)
- Adults suffer from more problems affecting the bone and gums around teeth (periodontal diseases) than teenagers.
- They sometimes have root canal treatments, broken, restored or missing teeth, dental implants or other forms of prostheses (crowns, bridges, partial dentures), which can modify tooth movement that can be done and the orthodontic mechanics that can be used.
- Nonetheless, the orthodontic treatment of such cases is possible, but requires a particular approach and particular treatment plans.
- Adults frequently have a “mutilated” dentition caused by the extraction or the loss of certain teeth, they have teeth that are more worn out and sometimes damaged, teeth that are tipped or have migrated (see pictures for examples) and suffer from more problems affecting the bone and the gingiva around the teeth (periodontium), etc.
- These conditions may lead to more complex treatments and it is often necessary to work in collaboration with the general dentist and other dental specialists to establish the best treatment plan with solutions coming from the different fields of modern dentistry.
To download a 5-pager from the American Association of Orthodontists on adult orthodontics (“L’orthodontie chez l’adulte“) (in French). The Damon® technique and protocols that we use are particularly suited for this type of treatment. The very slight forces, the easy maintenance and cleaning of the appliances, the minimized level of discomfort, the frequency of visits and a shorter duration of treatment for certain types of cases compared to the conventional approaches make this technique ideal for treatments in adults. The use of new anchorage mini-implants also opens new horizons in adult treatments by allowing us to offer options of treatment that were hard to envision only a few years ago. So, if you are healthy, if you have healthy teeth and periodontium (support tissues of teeth: bone and gum), there should not be any contraindications to envision an orthodontic treatment. Consulting a specialist certified in orthodontics (orthodontist) could confirm it quickly.
“Compromise” treatments

Adult with a “mutilated” dentition (cavities, fractured and extracted teeth). Orthodontics prepared the dentition so the dentist could make adequate restorations.
We have had patients from 3 to 81 years of age! Particular challenges come with each person, but adults often have particular expectations and demands when it comes to orthodontics. They have various motivations to start a treatment. Sometimes, a chronic functional problem that has become incapacitating convinces them to consult. In other cases, years of wear affecting certain teeth require orthodontic corrections to minimize future damages. However, despite the presence of multiple problems, some people only wish to correct the unesthetic aspect of their dentition that bothers them. For many reasons, adults often ask questions on the possibility to have a “compromise” treatment aiming at making a few corrections that are more “limited” compared to a “global approach”. Ideally, it is often indicated to make “global” corrections or perform a “complete” treatment aiming at maximizing esthetic and functional benefits and promoting a better stability of the corrections obtained. However, in certain types of cases, offering “alternative” treatment plans may be possible and constitutes some compromise compared to what would be considered as an ideal approach. For instance, this may be the case when a patient whose growth is finished (adult) shows a significant imbalance between the jaws and, for various reasons, does not want to or cannot undergo a surgical procedure that would be necessary to re-establish the balance between his/her jaws. In such a case, orthodontics can improve several esthetic and functional aspects of the dentition without correcting the position of the jaws or certain irregularities in the interdigitation of upper teeth with the lower ones. Limited corrections often have the objective of improving esthetics without nonetheless changing the function of the dentition that may be problematic. A patient’s perception of his/her dental problem may be quite different from the one an orthodontist may have, since he/she evaluates the dentition and the bite as a whole. For instance, someone may wish to only correct “one or two crooked” or prominent teeth. In reality, the malposition of these few teeth is due to a generalized lack of space that would require to move other teeth, which would affect the rest of the bite. Therefore, an evaluation must be done to determine if the negative side effects of limited corrections are more significant than the benefits to the whole dentition. Here are a few examples of orthodontic corrections that may be limited to certain parts of the dentition only:
- Closing of spaces between a few anterior teeth;
- Closing of a posterior space to avoid having to install an implant or a bridge where a missing or extracted tooth is located;
- Uprighting of tipped teeth to get ready to install a bridge or an implant (see farther down the page);
- Correction of simple rotations on anterior teeth (rotated teeth);
- Move a damaged tooth to allow the dentist to better restore it;
- Corrections of a few teeth to get ready for the installation of a partial prosthesis by the dentist;
- Correct anterior teeth only, sometimes to one arch only (upper or lower), but this approach is not always possible.
There is compromise… and compromise!

Certain compromises are realistic… while others are not!
People regularly ask us if it is possible to make limited corrections or undergo a compromise treatment during consultations. Often, patients only see one aspect of their problem without understanding how complex the required orthodontic corrections are in order to correct their problem and they do not have realistic expectations. The “classic” example is “one crooked tooth only”, a few prominent teeth, problems to one arch only, etc. Although we want to meet patients’ expectations as much as possible, it is often impossible to offer compromise options since what patients ask us is completely unrealistic, so it is better not to do anything! We offer several types of treatment that will respond to adult patients’ demands and particularities.
- The best way to find out about all orthodontic possibilities and the different options of treatment for a particular case is to come see us.
- Starting at the initial consultation, a preliminary evaluation will be done and you will get a good idea of the possible options of treatment, their duration, the related fees and if your condition is favorable to an acceptable “compromise” approach.
- ➡ To see other examples of orthodontic compromise treatments.

Example of a limited treatment with the goal to eliminate a problematic lower incisor. This woman is in her forties and she did not wish to get any corrections done to her upper teeth. (A and B) Before the orthodontic treatment, the lower right incisor had had a root canal treatment, significant wear (very short root) and bone loss (see D; pre-treatment radiograph). The prognostic of this tooth was bad in the long term. (C) After the orthodontic treatment and the extraction of the damaged incisor. Corrections were made to the lower arch only.
Orthodontic camouflage
Compromise treatments often require to “hide” a skeletal imbalance between jaws that are badly proportioned by dental compensations. To learn more on this subject and to see examples, consult this section on dental compensations or orthodontic camouflage. 
Loss of posterior teeth and uprighting of molars
- The loss of a posterior tooth (molar), a condition that is relatively common in adults, often leads to the tipping and migration of the adjacent and opposing teeth by allowing the other teeth to move toward the toothless space.
- Losing a tooth is never without consequences. Studies have shown that 50% of the level of bone that supported the tooth will be lost within 12 months following the extraction, from which 2/3 will occur during the first 3 months. Therefore, replacing the teeth is essential to preserve as much alveolar bone as possible. The loss of alveolar bone is cumulative and irreversible. (Schropp et al.)
- Following the extraction of a lower tooth, the upper teeth no longer have opposing contact and may get longer (extrusion) and the adjacent teeth may fall into the space.
- This may cause bad interferences between the teeth during function in the middle or long term, which may lead to tooth wear, broken teeth, functional or joint problems and the loss of the tissues that support the teeth.
- The loss of posterior teeth affects the occlusal height and may cause a posterior collapse. To learn more on posterior bite collapse.
- A recent study showed that extracting a lower molar on one side only will cause:
- a significant tooth movement toward the extraction site;
- progressive bone loss in the extraction area. This bone loss will increase with age. (World J Orthod 2010)
- The dentist may propose to the patient to upright the tipped teeth in order to be able to replace the missing tooth by a partial denture, a bridge or an implant.
- Therefore, orthodontic corrections aim at repositioning the teeth in the most ideal position possible in order to help the dentist perform his work afterwards, that is replace the missing teeth.
- The treatment may sometimes be limited to uprighting one or a few teeth in the affected area only.

(A) The uprighting of a tipped molar helps increase its functionality. (B) After the orthodontic correction.

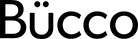
(A) A 50-year-old woman who lost several posterior teeth, which caused the tipping of the other molars throughout the years (arrows). (B) Orthodontics made it possible to upright the molars in a better position. This will help the dentist replace the missing teeth after the orthodontic treatment.
Uprighting molars may be indicated even if no tooth was lost as (A) in this teenager where the second molars are tipped forward and cannot erupt properly. These teeth are doomed in the middle term if they are kept as is because it is impossible to clean them and they will eventually develop decay. It is necessary to move the crown back and move the roots forward to upright these teeth (arrows). (B) During the treatment, the molars are repositioned and the whole surface of the crown is accessible for cleaning.

An extracted or missing tooth allows the other teeth to tip toward the space. This creates difficult areas to clean (arrows) where food and plaque may accumulate and cause irritation, inflammation and eventually gingival and bone loss. Uprighting tipped teeth makes it possible to minimize this destruction of tissues.
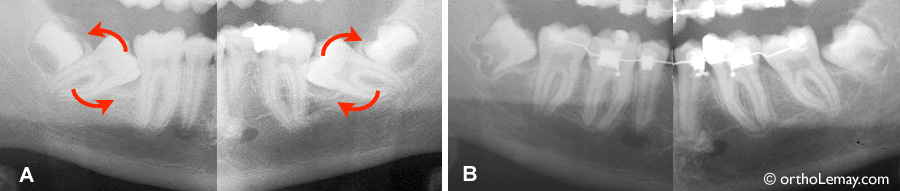
(A) Posterior teeth that tipped forward several years after a 46-year-old woman lost a molar. (B) The teeth were uprighted orthodontically by moving them backward (arrow). Once the space was obtained, another specialist (periodontist or surgeon) installed 2 implants to replace the missing molar. (C) Final result once the general dentist installed the crowns on the implants (arrows).

Loss of posterior teeth in an adult. On one side (A), the loss of a lower molar allowed the other molars to tip forward. On each side (A and B), the upper molars migrate toward the space below (extrusion). These teeth will ideally have to be repositioned to allow the dentist to better replace the missing teeth with a prosthesis.

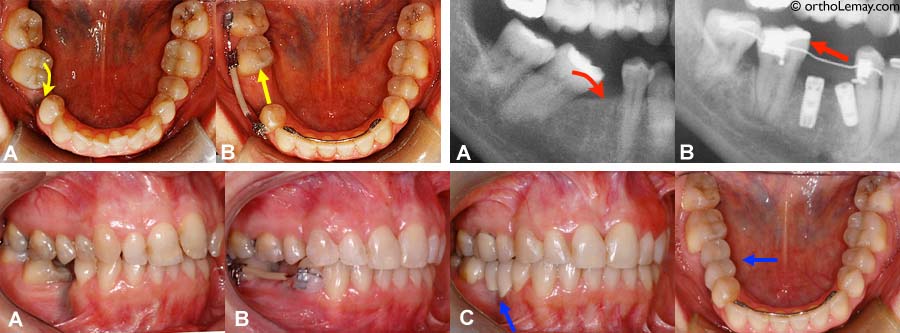
(A) Over eruption of upper teeth that no longer have support following the loss of lower molars. (B) Open mouth: the teeth have fallen so far down that they touch the lower gingiva (circle). (C) In addition to growing downward, the molars affected are tipped inward. Bone loss (periodontal disease) explains the presence of “black triangles” and the absence of interdental papilla between the upper incisors.

Example of orthodontic intrusion of a tooth that had “lengthened” (extrusion) throughout the years following the loss of a tooth in the opposing arch. The interarch distance does not allow the dentist to make an adequate lower prosthesis due to the lack of space. (A) Upper left premolar that has “fallen downward” and negligible space with the lower arch (yellow arrow). (B) Orthodontic mechanics used to “intrude” or move the tooth upward. (C) After intruding the tooth. (D) At the end of the orthodontic treatment, the available space (yellow arrow) now makes it possible to fabricate a lower prosthesis. Note: This 57-year-old patient had an upper removable prosthesis that replaced both upper central incisors. The prosthesis is not in the mouth on the final picture.

Example of extreme vertical movement of posterior teeth several decades after extracting opposing teeth without replacing the teeth by a dental prosthesis. (A, C) The premolars and a molar were extracted on each side of the upper arch, as well as the lower molars. Throughout the years, the lower premolars migrated upward, while the upper molars got “longer”. (B) Front view. The orthodontic corrections are now a lot more complicated!

Another example of orthodontic corrections in a 47-year-old woman. (A) The upper incisors are tipped backward and cover the lower incisors completely (Class II division 2 malocclusion). The vertical levels of teeth are easily seen when the mouth is open. (B) After the corrections, the inclination of the incisors is corrected and the lower incisors are visible, which also facilitates the function. (C) A view of the upper arch shows the change in incisor inclination and the shape of the arch. (D) Smile before and after the orthodontic treatment.
➡ To see cases of adults treated orthodontically and more complex interdisciplinary cases.
➡ Braces are also for adults; to read a text on adult orthodontics published in the La Presse newspaper (October 2014) (in French) in collaboration with the Quebec Association of Orthodontists. ➡ To read our blog column called “Un beau sourire n’a pas d’âge” (in French).
Share your orthodontic experience as an adult!
You are an adult and have undergone an orthodontic treatment? Share your experience by writing in the section below. Sometimes, several people like you hesitate to start a treatment because of unknown aspects that orthodontics represent for them. Even though we can give a lot of information to future patients, comments from people having undergone a similar experience are priceless for the orthodontic clients. Moreover, do not hesitate to ask questions.
Orthodontics for adults, a patient’s perspective If you are an adult with braces or considering orthodontics to straighten your teeth, visit Archwired.com, a website created by a mother who underwent 3 years of treatment, and dedicated to providing unbiased information and support.